Is it just me? Or are you feeling a buzz of invincibility from this honey? Read more in And now for something completely different …
A little housekeeping. It is Long Covid Awareness Month. Many of us will be thinking about those we have lost, and those who suffer with this currently incurable disease (about 40 million by some estimates). Please help out the cause in any way you can, even something that seems small, like informing friends about it, or preventing others from getting by promoting masking and clean air. Collectively, we can make a difference. Last year, I cohosted a 12-hour event with Becky Robertson while I had the damn norovirus. This year, she is going 24 hours with an all-star lineup of guests. Please join, you will not be disappointed.
There will be thousands of light displays that will light up across the globe. I will add a list of these in the next substack.
Hello again! I am getting better by the day. I am up to about 600ft (183m) of walking distance, can hop up and down stairs, and my arms are bulging because I can only put weight on 1 leg. That should be another month, then I expect to be able to put weight on it. Enough of me, too much to cover today.
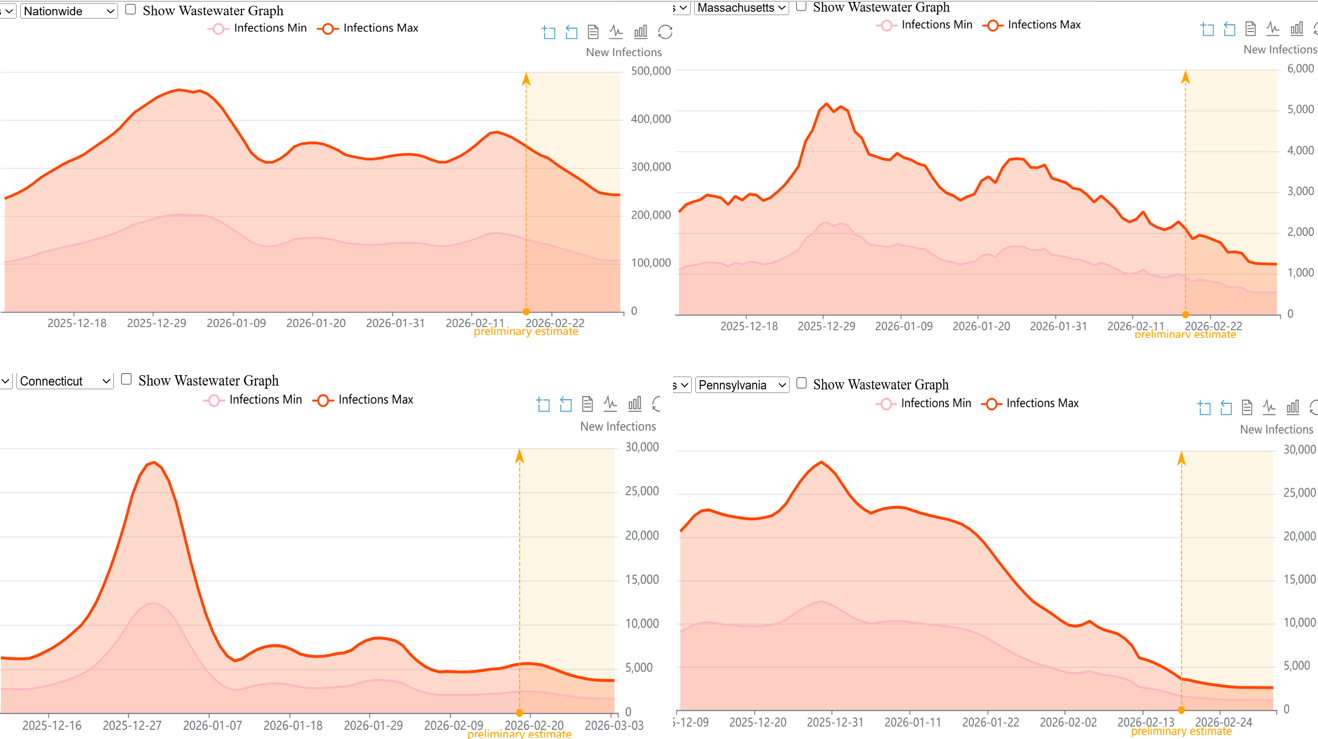
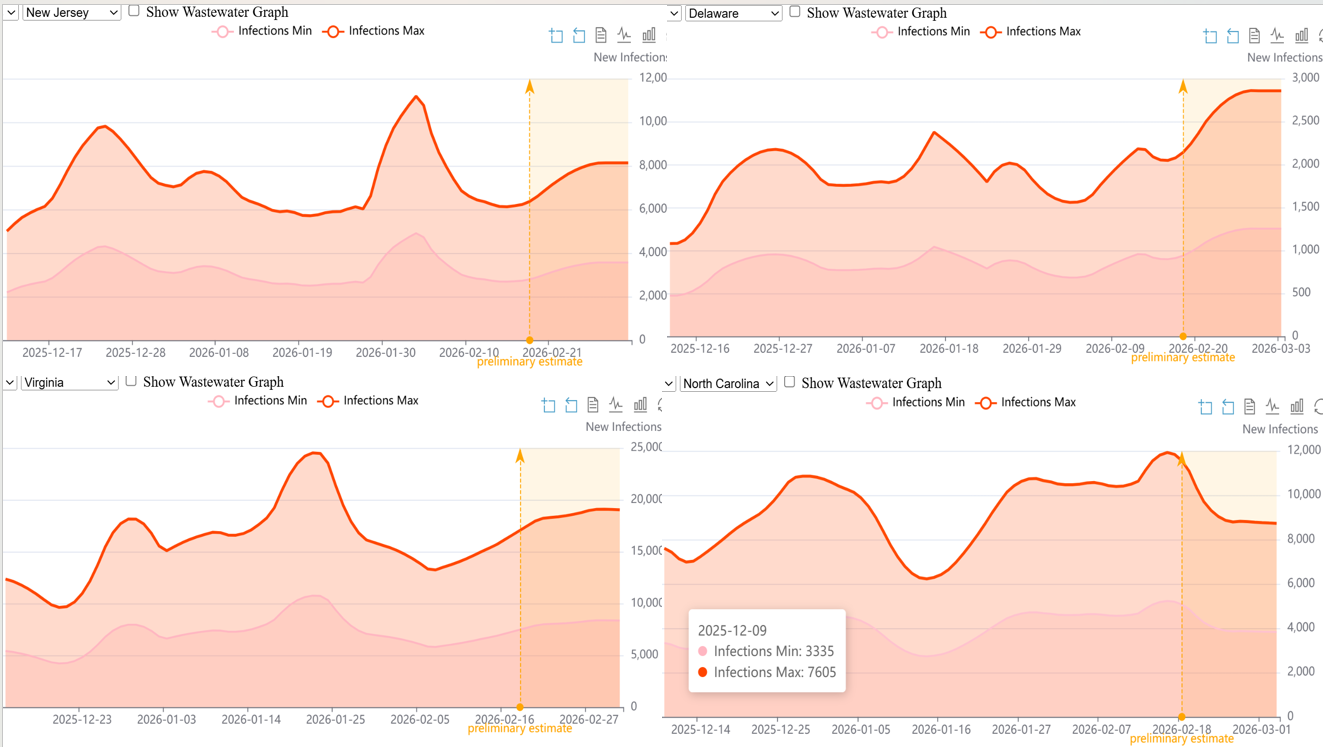
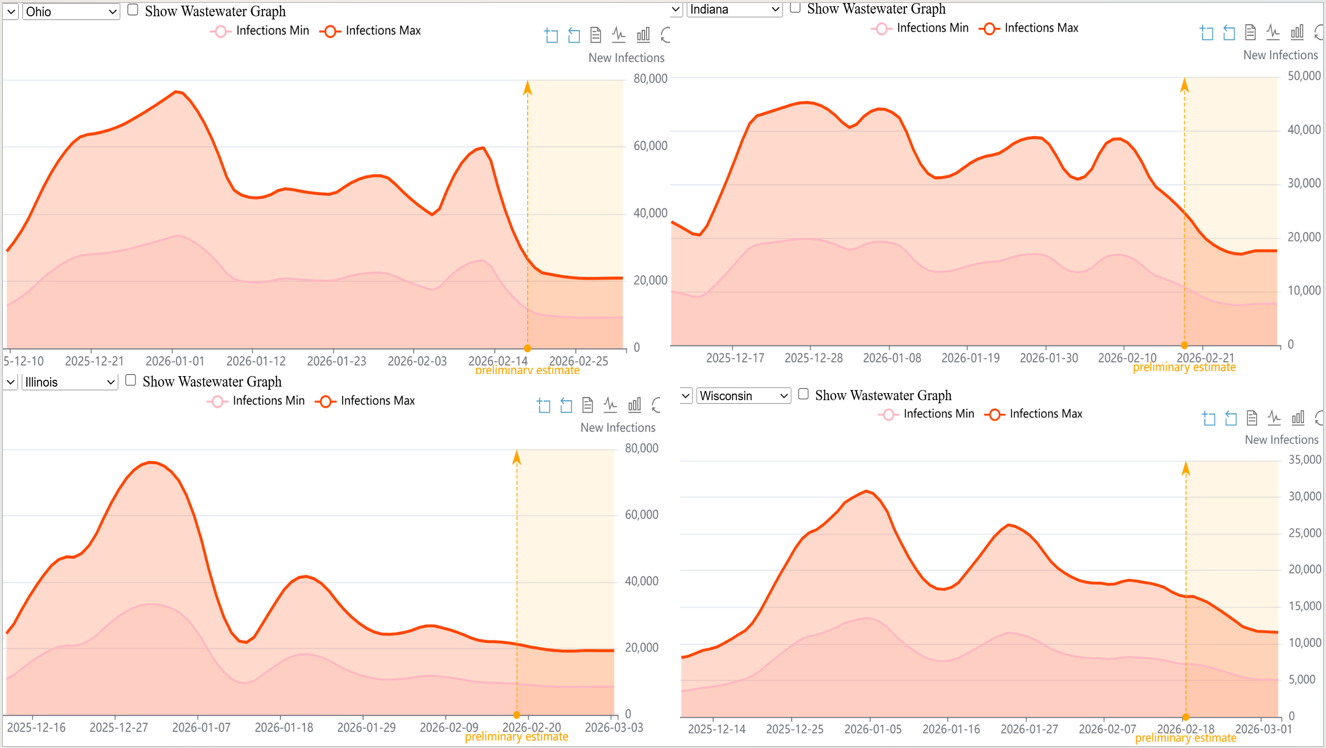
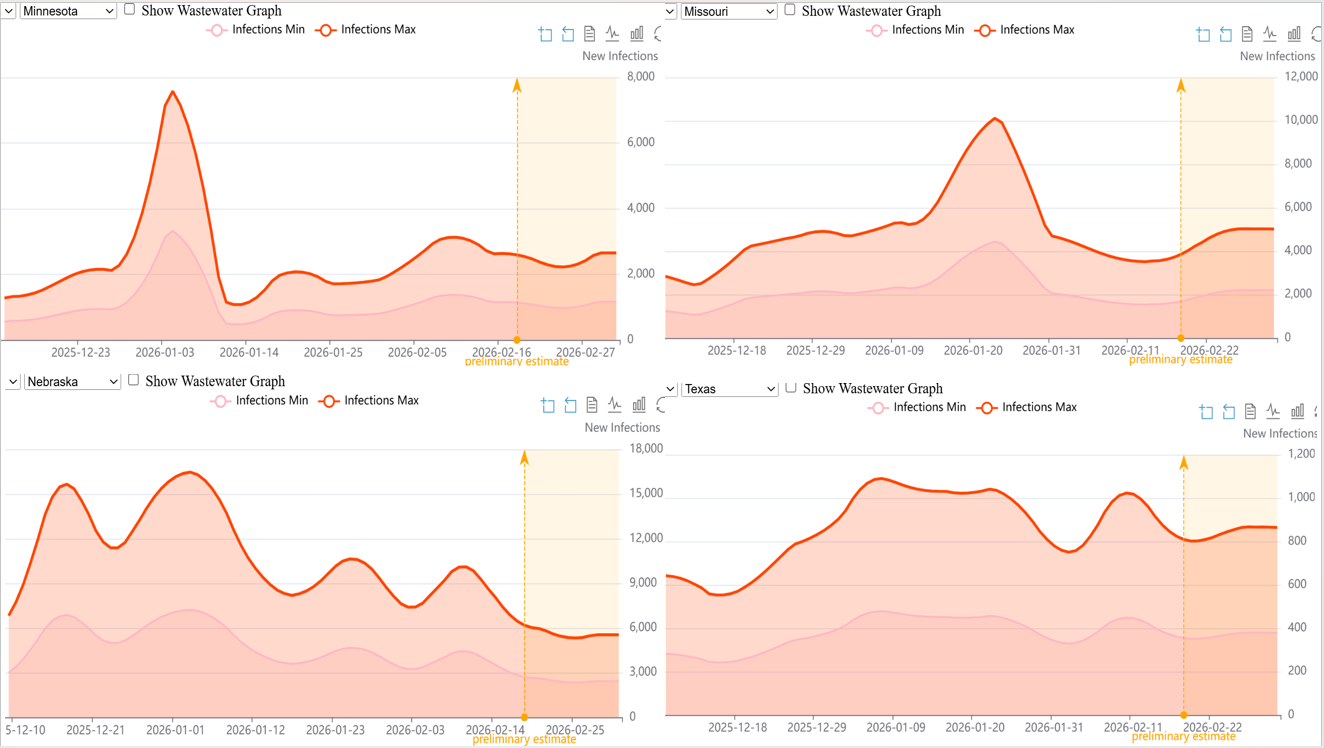
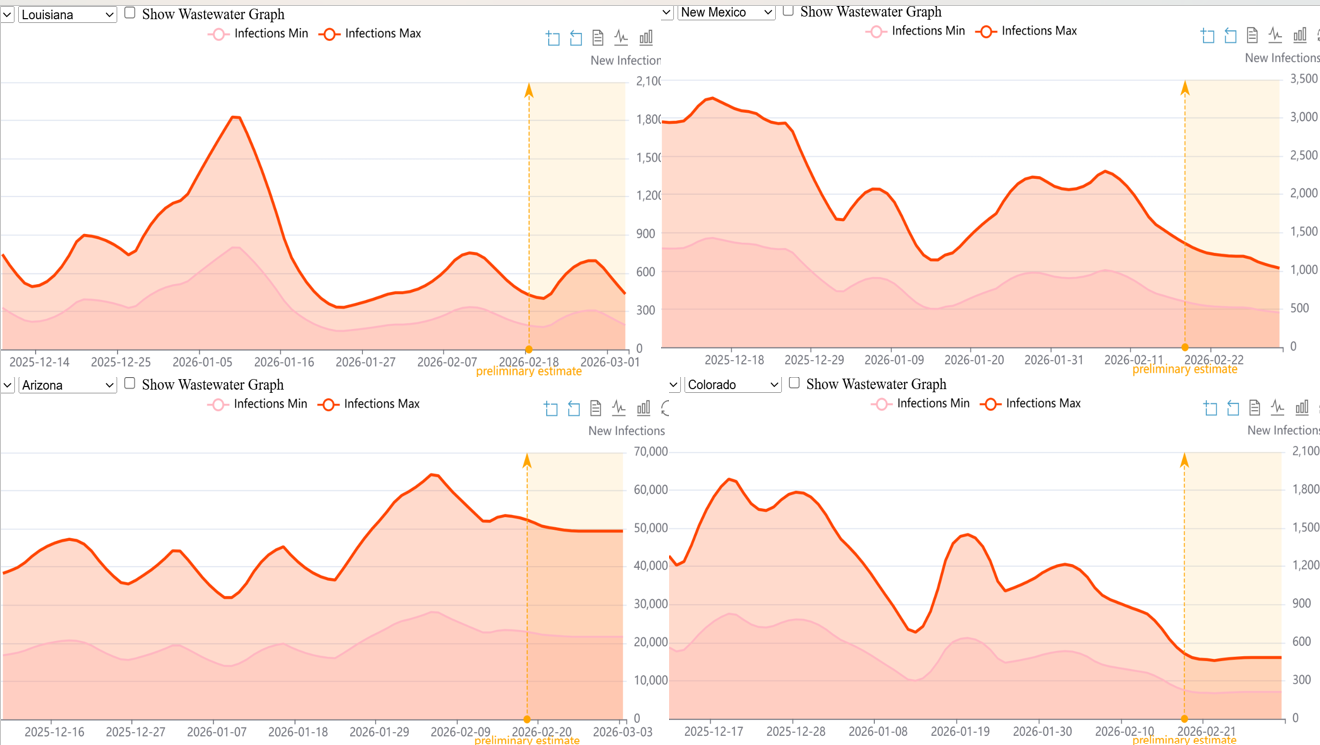
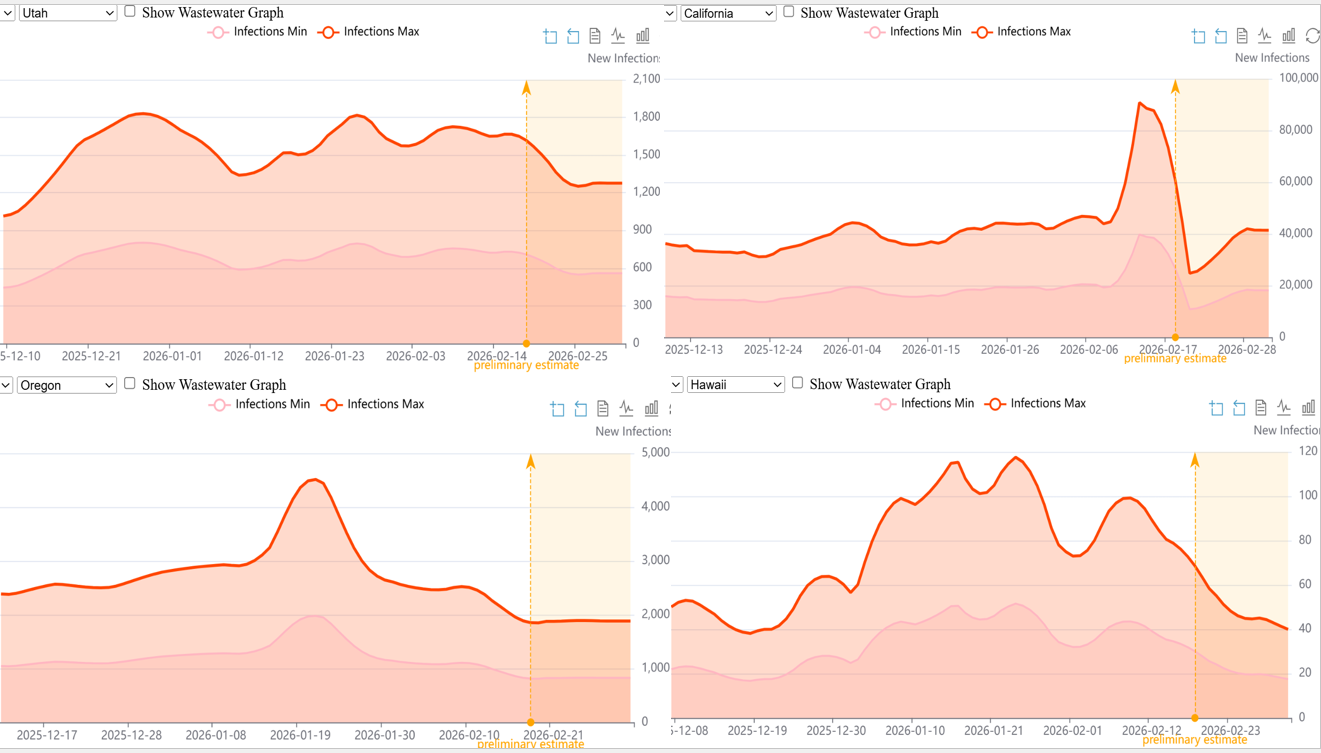
Let’s first get caught up on wastewater-derived New Daily Infections (NDIs). Here is a series of plots by state and nationwide. We relaxed our inclusion rules, and there are now 26 states included on our plot page at the WHN. The following states are in decline: MA, IN, PA, CT, NY, HI, NM, NC, WI, UT, OH, and the USA. Meanwhile, NJ, DE, VA, and MS are increasing. Finally, CO, OR, IL, AZ, MN, TX, LA, and NE are holding steady. There are two states that don’t know what the hell they are doing, CA and OK. The preliminary estimates begin 2-18 and extend through 3-3-2026.
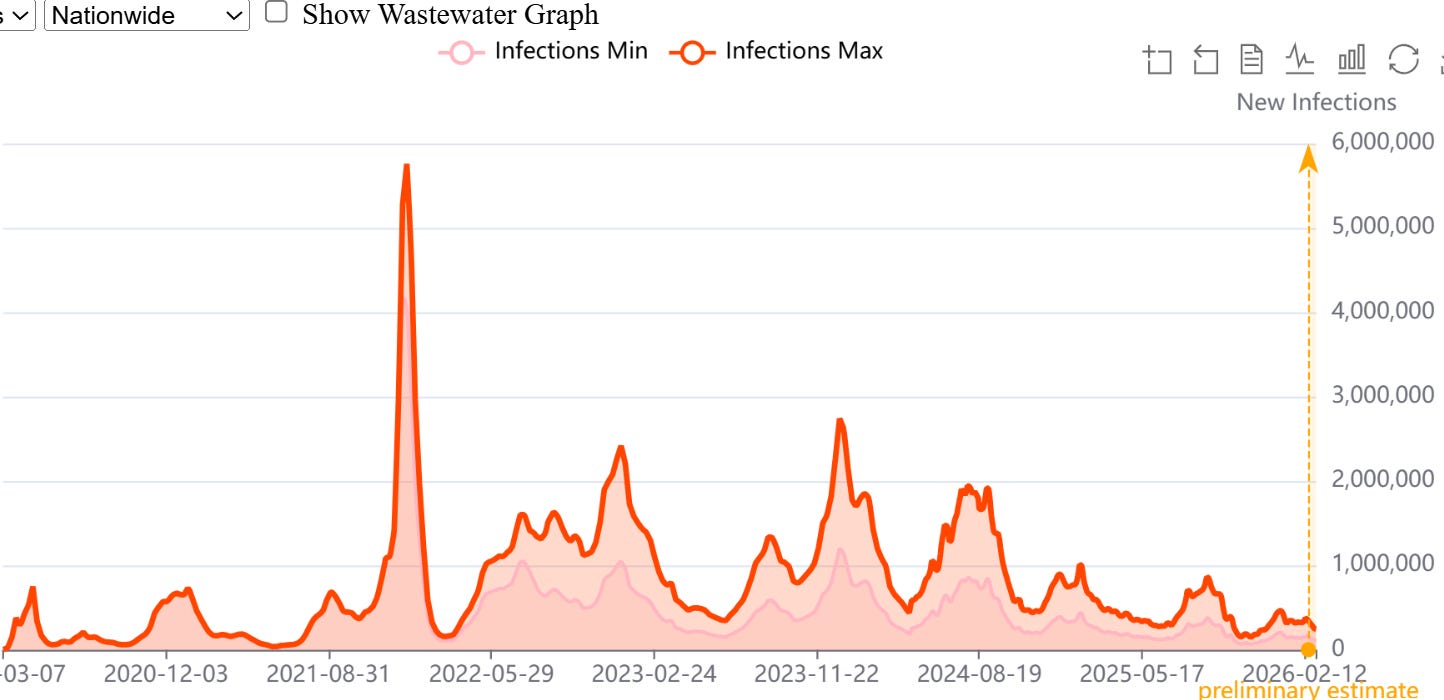
We also need to put the current wastewater-derived NDIs in perspective. Look how low, in a relative sense, 2025 and 2026 (so far) have been. I doubt we will ever see something like the first Omicron wave (~6 million NDIs) again. There appears to be a trend towards decreasing waves. Frankly I am not surprised, and I will explain shortly.
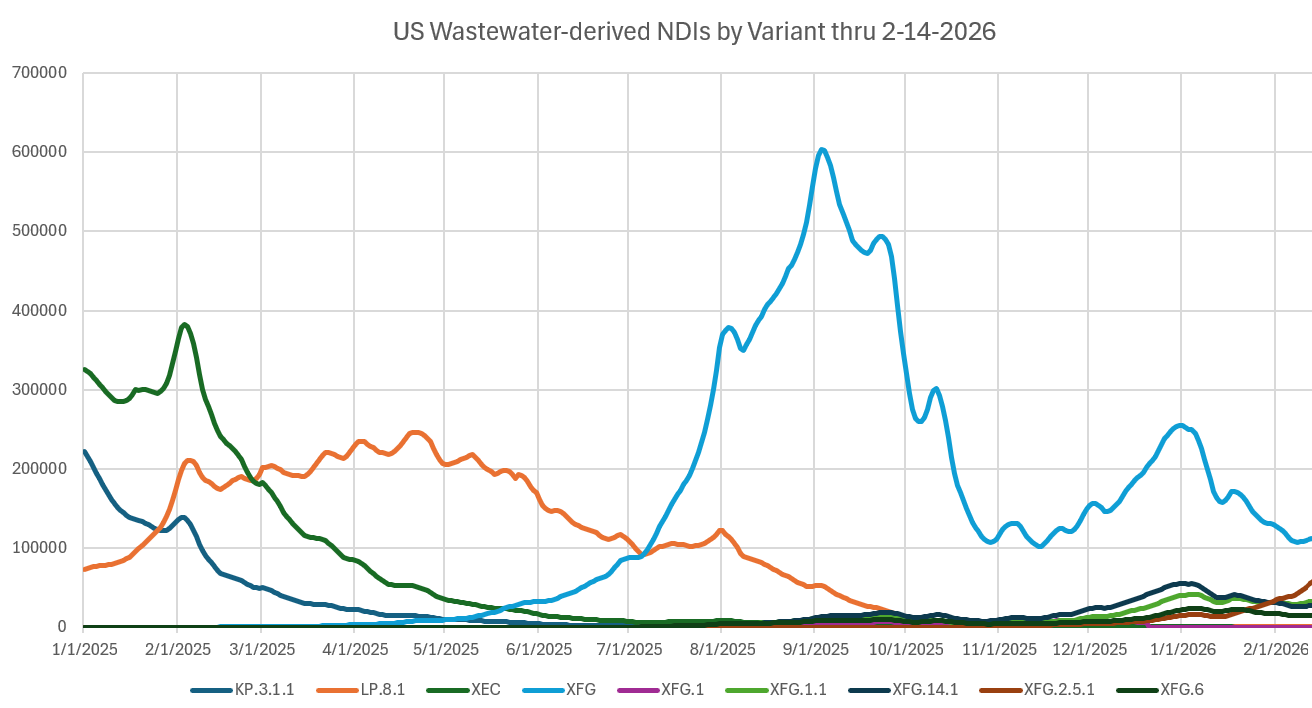
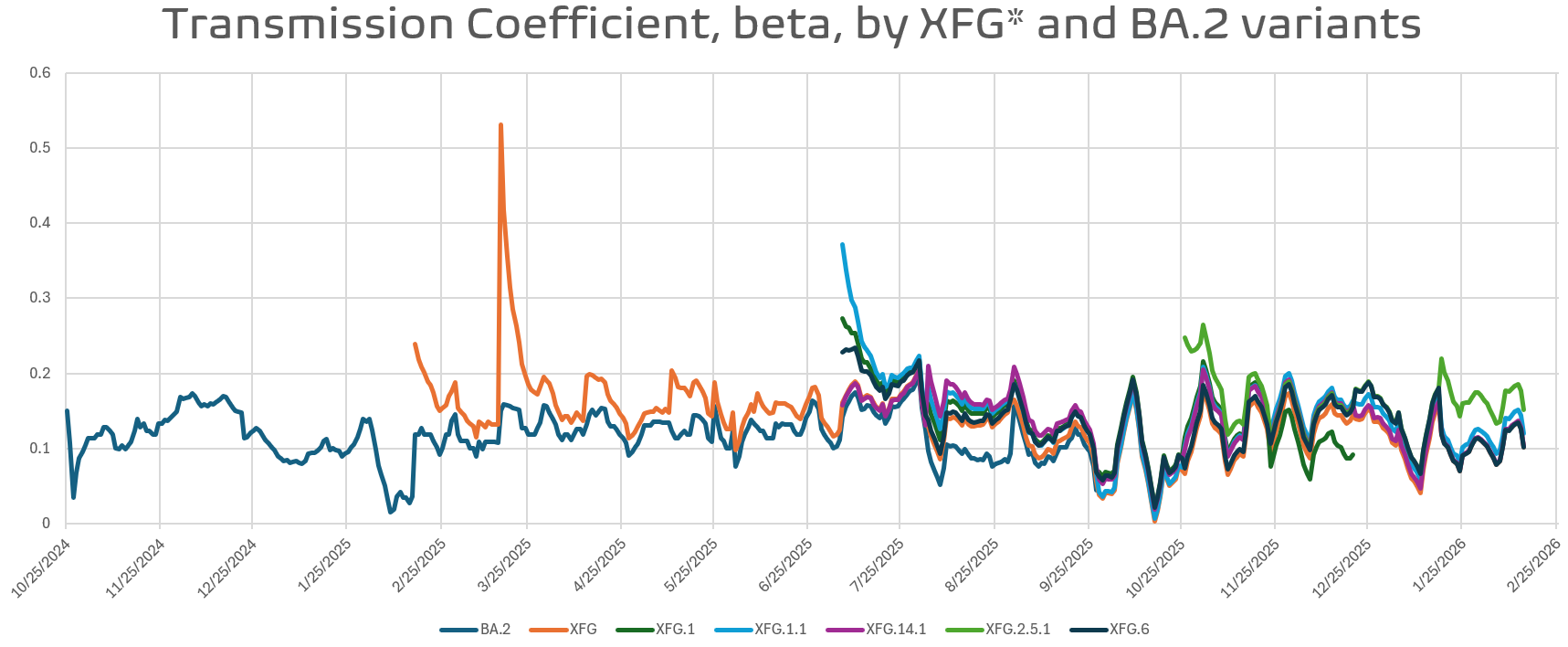
Let’s go back and look at 2025. What was going on there? XEC was dominant early, with KP.3.1.1 and LP.8.1 taking over the top spot. In the meantime, Nimbus, NB.1.8.1, and Stratus, XFG, were lurking in the background, battling between the two to see which would emerge. As we all know XFG emerged from this skirmish and its dominance has lasted nearly 9 months, surpassing BA.5. However, there is a price to pay for such a long run. Nearly all people who have been infected over this long period have natural immunity to XGF and all of its different flavors, and let me tell you, it is like the Baskin-Robbins of variants.
I calculated the transmission coefficients, β, and plotted the XFG flavors and BA.2. Currently, when Immune Escape and ACE-2 binding affinity (ba) are calculated, they are displayed relative to BA.2. Many interpret ACE-2 ba as the strength of the transmission and think β. I do not believe this is the best interpretation. The reports I have seen have XFG ACE-2 ba as less than half of BA.2. After seeing this, and repeated for other variants I will no longer use it to automatically set other variant parameters. Remember, MAPS used ACE-2 and IE to form ratios and ACE-2 was used for β, while IE was used to adjust reinfection coefficients, waning period length, and a few other parameters. I am shifting to a straight β(t) and relative growth advantage in the future.
Speaking of MAPS, I have some exciting news as I transition from MAPSV2R to MAPSV3. I have developed an entirely unique compartment model that should deliver incredible computational performance, higher accuracy and no negatives through a Strong Stability Preserving Runge-Kutta (SSPRK3) time-step scheme (4 sub-timesteps). The most important addition is the Leonardi effect, which we will discuss shortly. With the addition of the Leonardi effect, I will also routinely include Influenza A/B, RSV, Pertussis, Measles, and TB. I will be finalizing the code when I get home next week.
Remember when I went over the Leonardi effect a few Substacks ago? Well, let’s here more in his own words, please subscribe to his newsletter. Here we go, from A.J.:
Somehow in the argument of whether we should avoid SARS Cov 2 infections, it was proposed that people may be worse off by not gaining immunity via infection to viruses. It went as far as some suggesting since we have been infected with viruses all this time in evolution, that we may be missing benefits or necessary immune education. This emerged as a cynical elaboration to the hygiene hypothesis, which posits that beneficial bacteria prevent autoimmunity and benefit the immune syndrome.
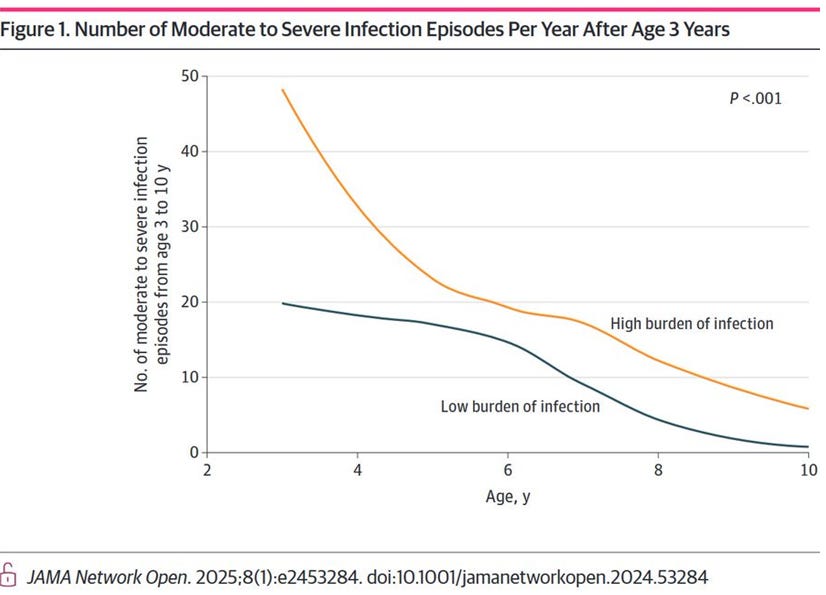
The recent hypothesis is a kind of apologism for infection, but nevertheless, deserves analysis. A recent study allows for such an analysis in a correlative way. The study split children between frequently infected and less frequently infected. Also, and this is important, individuals that were immunocompromized were excluded from the study. This is important because it is expected that immunocompromized people will not gain immunity from infections to the extent that immune replete people would.
The bold was my emphasis.
What is interesting is that the study found that individuals with less frequent infections in childhood also had less frequent infections in adolescence. Individuals with frequent infections in childhood had more moderate and severe infections than the other children in adolescence but also infections decreased compared to when they were younger.
This graph shows it rather succinctly.
We can say this corresponds with a facet of knowledge of immunity: In childhood we are frequently infected with bugs and this decreases with age and experience. However, it challenges the notion that each infection caught earlier staves off later infection in equal measure and reduces the severity. Instead, those with frequent infections continued the trend. What does it mean? That there is not a dominant effect of the number of infections conferring an immunity benefit. If there were, and if the effect were dominant, then we would have seen that individuals with frequent infections early in life would have fewer infections later.
It also means that severity of infections is not a function of novelty, but rather intrinsic from the immune system. There remain two hypotheses of why infections were more frequently severe later in life in the people frequently infected in childhood
1. That despite removing immunocompromised individuals from the cohort, there is some kind of immune problem these individuals had to begin with
or
2. Frequent infections predispose to severe disease by virtue of aging or dysregulating the immune system
We will address this topic later, but my hypothesis is frequent or sustained immune activation can lead to decompensatory or poor responses later on.
Yours,
AJ
With that said, now think about SARS-CoV-2, and how it is basically a machine that enhances AJ’s hypothesis to a level never seen before for an airborne virus. Sure, its entry point is the respiratory tract, but it is a vascular neurotropic disease, make no mistake about it. Do not call it a respiratory virus!
Now back to the Leonardi effect and why I think it so important to include in my pathogen model. First, the basics of his effects as related to SARS-CoV-2, not quoted verbatim, but as I understand them. First, what we just saw:
Repeated infections produce additive immune system stress, gradually degrading immune function.
Each infection will worsen immune dysregulation rather than simply boosting immunity.
And there’s more:
SARS-CoV-2 infection alters T-cell function, number, and survival.
It disrupts immune coordination and may cause abnormal immune responses.
Hyperactivation leads to premature aging and exhaustion of T-cells, reducing their long-term effectiveness.
Persistent immune activation may damage organs and impair immune regulation.
SARS-CoV-2 infection can cause lymphopenia (loss of lymphocytes) and reduced naïve T-cell reserves.
This may reduce the body’s ability to respond to future infections.
Persistent antigen exposure can maintain long-term immune activation, contributing to long-COVID and systemic inflammation.
Immune-mediated injury and inflammation may occur in the lungs, heart, nervous system, and other organs.
I think you got the idea, and it’s not a pretty picture. I might go into more detail at the cellular level in a future Substack and talk about one of my favorite subjects: SARS-CoV-2 and the mitochondria.
Now, why is this important in the model? In its most basic form, the model will accumulate this effect and allow for increased infections from not only SARS-CoV-2 but also other pathogens, like those I have listed. Remember, it is not going to be airborne pathogens exclusively, but will include molds, fungi, and bacterial pathogens. Think of as this basic model:
SARS-CoV-2 infection → immune hyperactivation → T-cell dysfunction/exhaustion → cumulative immune dysregulation → increased vulnerability to disease and chronic inflammation
At this point the only folks that don’t accept this are the dinosaurs in the field. He was castigated and chastised, but in the end it is the deniers that need to eat some crow, an apology would be to much to expect from that crowd/ .
And now for something completely different …
I need to find some of this sweet sticky shit. YUMMY! I always knew honey was a good anti-microbial, but never knew some was better than others. This is COOL!
Honeybees collecting nectar from a "buffet" of Australian native plants made honey with anti-microbial abilities that is more potent than "single origin" honey made from only one source of plant or flower, a University of Sydney-led study has found. The findings could help develop new treatments for drug-resistant infections while supporting bushfire recovery and sustainable beekeeping practices across Australia. They also place native Australian honey as a strong competitor on the global landscape.
The World Health Organization has declared antimicrobial resistance one of the top 10 global public health threats facing humanity, driving interest in the medicinal value and potent antimicrobial activity of honey. Reports of critical antibiotic resistance in Australia increased by more than 25% in 2024.
It turns out that plant diversity helps produce high levels of bioactive compounds needed to give the anti-microbial boost! I have been using more honey in my cooking instead of sugar; now I want some from Australia.
Be kind to yourself, and please be active for Long Covid Awareness Month! I will try to publish another Substack tomorrow. We’ve got a lot happening on this planet. H5N1, Measles, and much more.
Take care,
Joe
I should be wearing a mask for my emoji on X, but I was in the middle of a lake when I took this.