


Mommy, I want this! Daddy, I like that? Well, you cannot have it all, my child. Children need this and that all the time. So when do they stop? Read more in And Now for Something Completely Different …
I apologize for not posting more often. I have had some health issues I have been dealing with for the last 2 months. Nothing serious, though. Just that darn little thyroid was so out of whack, I had zero energy to do anything. Thanks to my doctor, we are now operating within normal parameters.
So now, get ready for a big dump of information with more to follow later this week.
Here is an interview I did last week on The Matt McNeil Show. Matt McNeil interview
In an exciting development I have been apointed as a WHN science experts advisory team. You can see a short bio here. I am truly honored to serve on this incredible team for the WHN.
SARS-CoV-2 and MAPS update
My gosh, where to start? Let us rewind to June 21st, 2025. Why then? Because that is the last date I ran a MAPS forecast. Here is a line graph of how well it performed.
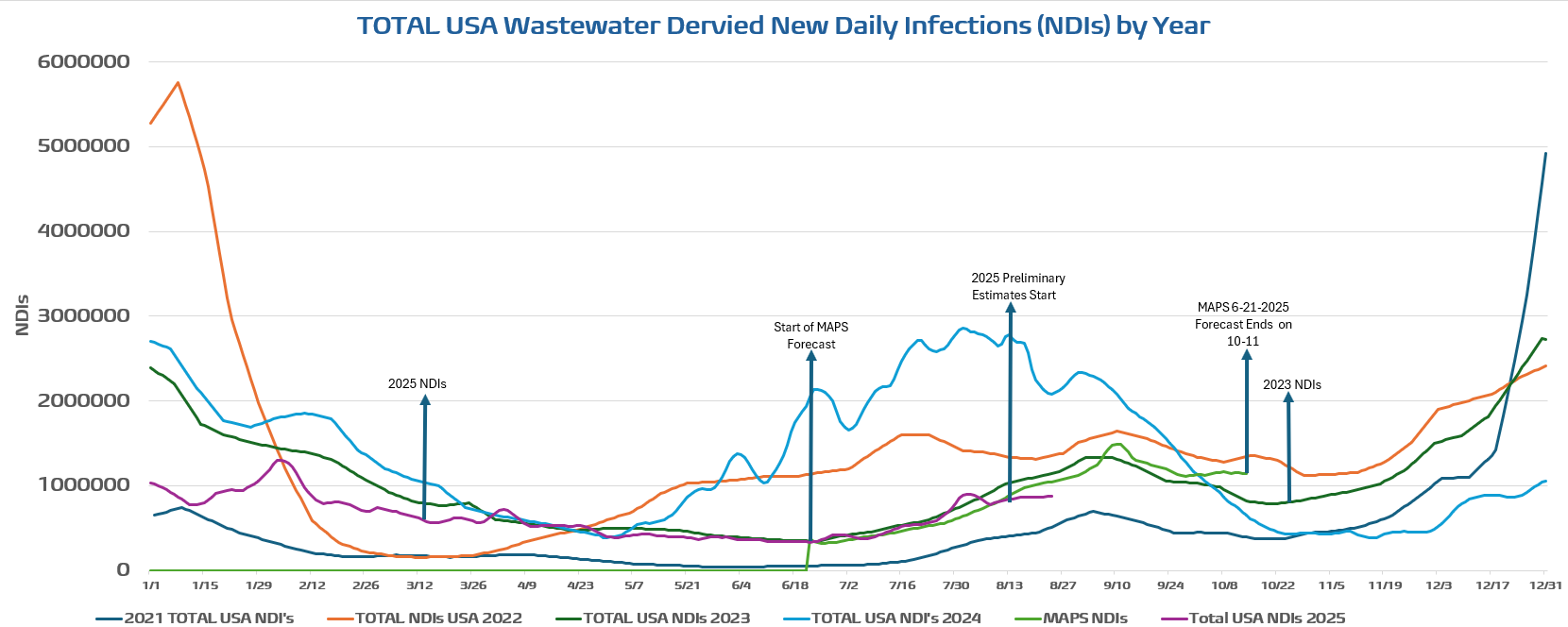
The graph indicates outstanding agreement between 2025 and the MAPS forecast for nearly 2 months, with MAPS showing a few secondary maxima/minima. Remember that the wastewater comes in 1-week intervals and is linearly interpolated between weeks, while MAPS is output daily. I will take this agreement any day that I issue a forecast.
The other years are plotted to illustrate that each year has a unique trajectory, driven by different variants and a developing history shaped by changing mitigation procedures, such as masking, vaccination efficacy and uptake, yearly weather variations, and evolving public behaviors, among other factors. I highlight 2023 and 2025 due to the similarities in their temporal patterns. Why is this similar? I believe it is due to the variant evolution in their types. If you recall from past newsletters, I called 2023 the year of the recombinants. Recombinants are derived from the exchange of genetic material between two different viral genomes within the same host. In coronaviruses, it is commonly referred to as homologous recombination because the viral sequences line up well, as well as the fact that these types of viruses have “proofreading” polymerases. Segmented viruses, such as H*N* or influenza, undergo a reassortment process where entire genome segments can be swapped around.
It turns out that 2025 is also what I would term the year of recombinants, too. In 2023, an amazing “soup” of recombinants emerged, and none could get a dominant foothold, likely due to similar immune escape, transmissivity, or similar traits in general. The XBB.1.5* recombinant (BA.2.75+BA.2.10) first appeared in October 2022 and wreaked havoc well into 2023, followed by an incredible number of recombinants that emerged. Things changed in August of 2024 when BA.2.86 emerged; it was not a “novel” virus, a newly identified virus in humans different from previously identified existing viruses (eg., Wuhan, Alpha-B.1.17, Beta-B.1.351, Gamma-P1, Delta-B.1.617.2, and Omicron-B.1.1.539), because it emerged from Omicron (like BA.1, BA.2, JN.1, KP.2 …). Still, in a loose sense, it was due to the extremely high number of spike protein mutations. Because it was a sort of “novel” virus, the population has little resistance to it. This was followed by JN.1, and KP.*, which continued to dominate into mid-2024. We then encountered another new recombinant, XEC (KS.1.1+KP.3.3) in June of 2024. This led to a record late summer/early fall wave that imparted enough natural and hybrid immunity to lead to the least severe winter/holiday wave relative to the three previous years. In late January 2025, a new recombinant emerged, XFG and XFG*, which are now creating the surge we see in late summer. NB.1.8.1 is now only a minor player on the world’s stage. We now have another potential pseudo-novel variant, BA.3.2, a far-removed Omicron lineage, that has started to ripple in different portions of the globe. The BA.3.2 sublineage of Omicron, or BA.3, possesses over 50 spike protein mutations relative to its ancestor and was first identified in South Africa. It made a brief appearance in the United States in early July, and I am confident it could emerge later this year in another form of recombinant. Relative to LP.8.1.1, its immune escape ability is roughly 4 times higher, while its ACE-2 binding affinity is a fraction of LP.8.1.1. You should now understand why 2023 and 2025 appear so similar.
A little more history is needed to explain why the last MAPS forecast was conducted on June 21, 2025. Much of this is due to the mismanagement of the Trump Administration and its impact on our health institutions. We first noticed an unexplained “freeze” of wastewater data back in January. The data then began to come back about a month later, but the data feed rate is just a fraction of what it used to be. This continues to be the case and has come to the point that the CDC decided to release its new variant proportions analysis in August, noting that instead of providing this in two-week intervals (there was a time it was weekly, but that began to change under Biden in May of 2023 — the end of the emergency declaration for SARS-CoV-2). We had over a 2-month gap in the variant proportions data that is used to initialize MAPS, in addition to the wastewater-derived infections we developed at WHN.
While the CDC was busy spinning its wheels in neutral, we decided to develop our own product. We have tapped into the GISAID database that tracks the SARS-CoV-2 variants. We will release this product formally in the coming weeks. In contrasts to the CDC variant proportions data, which contains 133 variants, our new product will contain 568 and more in the future. Here are tables of the variant proportions for the CDC in June and the new table from August.
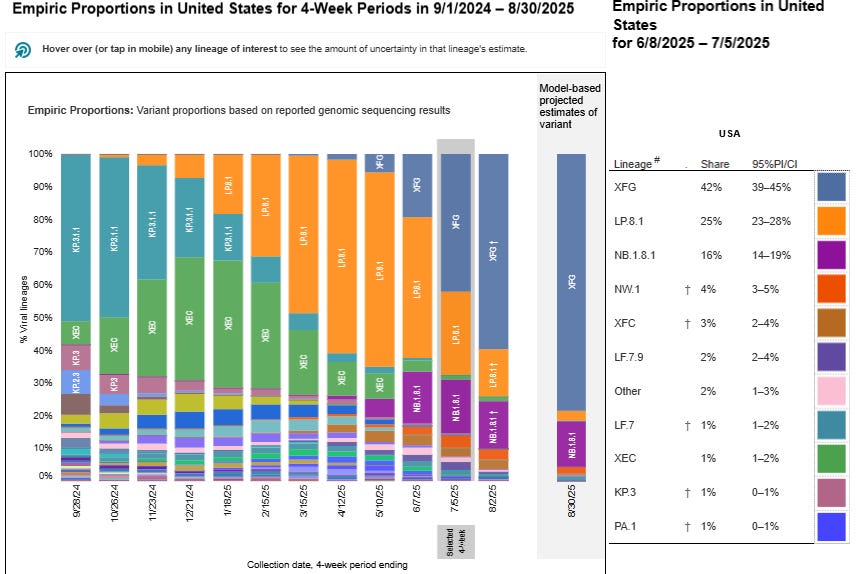
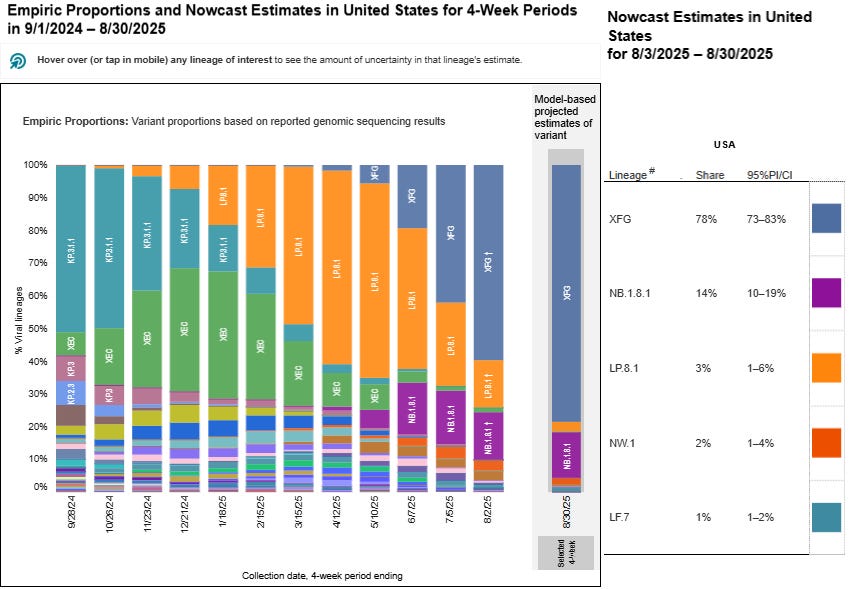
Oh, darn, they look the same because they are the same on the left-hand bar chart. Um, I think they F’d up. The bar charts do show the progress (in 1-month intervals, now). Back when I was doing the last forecast, XFG and NB.1.8.1, along with the declining LP.8.1, were in a battle for dominance. NB.1.8.1 was dominant in California, XFG was dominant in New York and the USA as a whole. Here is an example from our wastewater-derived NDIs combined with our new variant proportions to produce NDIs by variants for New York, California, and the USA. The end date is 8-13-2025.



Although NB.1.8.1 is dominant in the California graph, adding up XFG.* reveals it as the dominant variant by the end of the time period. Of the XFG sublineages, XFG.3 is the most prevalent by the end of the time period. You'll notice we now offer more flavors of the XFG recombinant. This feature is beneficial, but it also poses a challenge for me, as I find it difficult to determine the Immune Escape (IE) and ACE-2 binding affinity for each subvariant to initialize the model. This is why I have not fully implemented the new GISAID variant proportions data in the model initialization. I am working on this. For now, I will use the CDC variant proportions data like before and issue a forecast later this week. The plan is to double my forecast ensemble from 20 integrations to 40 integrations by using the CDC and WHN variant proportions datasets. This will theoretically improve my forecasts. It will also involve considerable work to go back historically and evaluate this new approach with observational data. Eventually, all of this will be posted frequntly on the WHN website.
And now for something completely different …
As many of us know kids seemingly want something all the time and it can really test your patience. It turns out that patience is the key. So keep that in mind before you make a comment you will likely regret.
Quitting time: Neurons that drive sociable behavior in children and teens turn off in adulthood Here are few takeaways from a ground breaking study at Yale.
Pediatricians and parents—and, really, anyone who works with children—have long known that a child's social needs evolve with age. Yale researchers have now discovered the neurological signaling that marks this process.
In experiments with mice, researchers observed that Agrp neurons, a type of cell in the brain's hypothalamus region, play a key role in controlling social behavior in young animals but not in adults. The neurons—which regulate primary survival needs like hunger and maintaining body temperature—drive social needs during youth but slowly lose this role in adulthood.
The findings illustrate the importance of social interaction in developing mammals. They also shed new light on how this need is biologically regulated and why it changes as we age and may help scientists better understand developmental social disorders in humans. The study is published in the journal Current Biology.
The summary further elaborates on the experimental methods.
In their work, researchers measured Agrp activity in mice at different ages, from weanlings through adulthood. Specifically, they sought to observe how Agrp activity would be affected by social connection with others, and if the correlation changed over a lifecycle.
In a series of experiments, the researchers measured Agrp activity after socially isolating mice and then after reuniting them with other mice. They used methods like calcium imaging, which tracks calcium ions to understand neural signaling and communication; and optogenetics, which uses light to influence neuron activity.
They found that social isolation strongly activates Agrp neurons in juveniles, and that social reunions bring their activity back to low levels. But when researchers silenced the Agrp neuron activity in young, isolated mice, the mice were less social overall. Reactivating the neurons renewed their social impulses.
In adult mice, however, none of the Agrp manipulations had any effect, leading researchers to conclude that while these neurons help regulate the drive for social contact during development, the effect stops in adulthood.
Honorable mention: Cats can get dementia too. Here are the eight signs to look out for

I have given you a lot of information for now, so I will stop at this point. I want to provide you with detailed updates on H5N1 (starting to pick despite the trickle from the USDA/APHIS data), measles (still occurring and school is back in session), MPOX (on the rise), and our old friend the Screw Worm (on an upwards trajectory). I will also provide my thoughts on RFK Jr and the shambles he has created at our national health institutions, as well as the state of vaccinations under this administration. The next newsletter will be published this weekend. Thank you for reading and your patience during my absence.
In the meantime, stay safe, and do kind acts for others and, most of all, yourself. Thank you for reading.
Joe
Miscellaneous items you might like are below.
Here are my new Facebook and X profile pictures.

Next up will be a weekend forecast with the latest CDC variants proportions analysis with some new goodies for you.
Here is a kick-ass at-home test, nearly equivalent to a PCR test.

SARS-CoV-2 is a vascular virus, not just a respiratory virus. To make it simpler for folks, call it a whole-body virus. No organ is spared. It infects our entire body and creates reservoirs throughout. It should be thought of as a Long COVID virus and will exploit pre-existing risk factors.
Check out this article. I love it. It’s an easy read but stimulates the brain in many ways.
Viruses Finally Reveal Their Complex Social Life - Quanta Magazine
Where do viruses hide in the human body? | The BMJ
Understanding immunity and viruses through the John Snow Project
Variant tracking at the CDC
Infections at WHN (updated!)
The neuroinvasiveness, neurotropism, and neurovirulence of SARS-CoV-2: Trends in Neurosciences (cell.com)
Dr. Joe, thank you for this excellent update--dense with content but clear and detailed. Considering your observations about all the recombinant variants this year, would you offer any thoughts you may have about the recently approved vaccines for 2025-26? I see Moderna has two, one being a brand new mNexspike vaccine that, I believe, targets a smaller segment or section of the spike protein and also results in a dose that is about one-fifth that of the previously and still available vaccine. Any thoughts as to whether this new vaccine might be preferred as to either efficacy or lower side effects? I think the testing to date found it essentially comparable as to efficacy but what I have read is limited and I am no expert (just a deeply concerned senior who believes in science and values expertise). Thanks!