

Pathogen Update: 9-12-2024
New Forecast, and Daily Feed of Brain Damage (Part II)

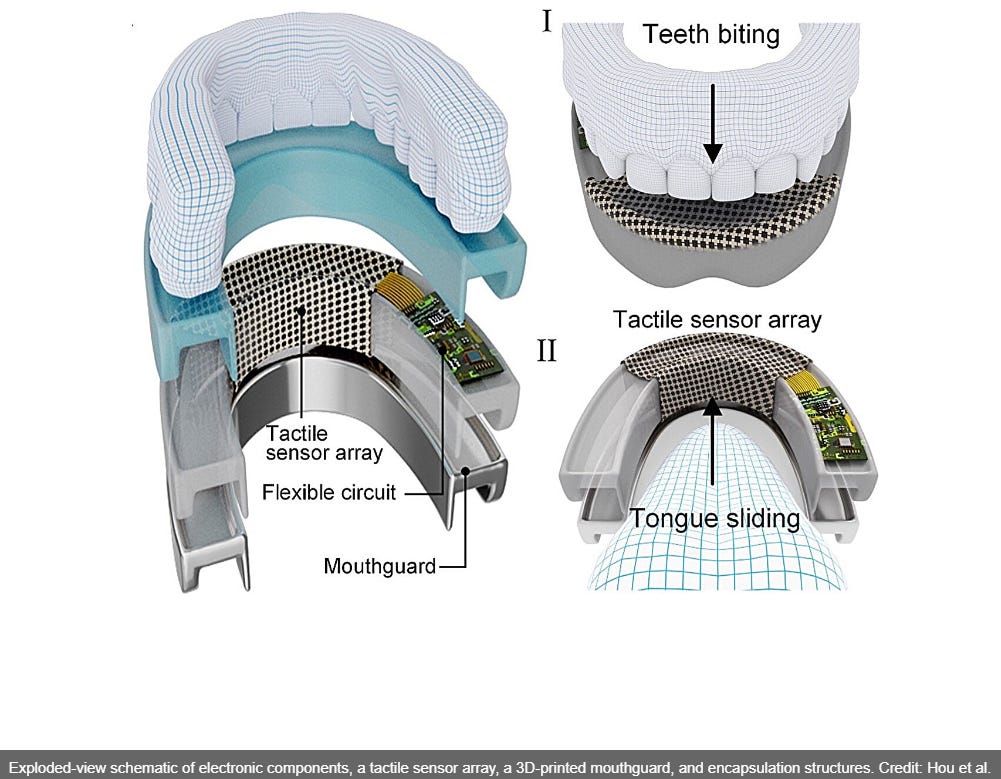
That’s so easy I could do it with my mouth closed! Read more in And now for something completely different …
Keep reading with a 7-day free trial
Subscribe to Dr. Joe's Covid and Science Newsletter to keep reading this post and get 7 days of free access to the full post archives.